Blood pressure is a measure of the force that blood exerts on arterial walls as the heart pumps it through the body.
Every blood pressure reading contains two numbers, expressed in millimeters of mercury (mmHg) and written as a fraction, such as 120/80 mmHg.
Both numbers matter clinically, and neither should be ignored when assessing cardiovascular health.
What is the difference between systolic and diastolic blood pressure?
Systolic and diastolic pressure represent two distinct moments within a single heartbeat cycle.
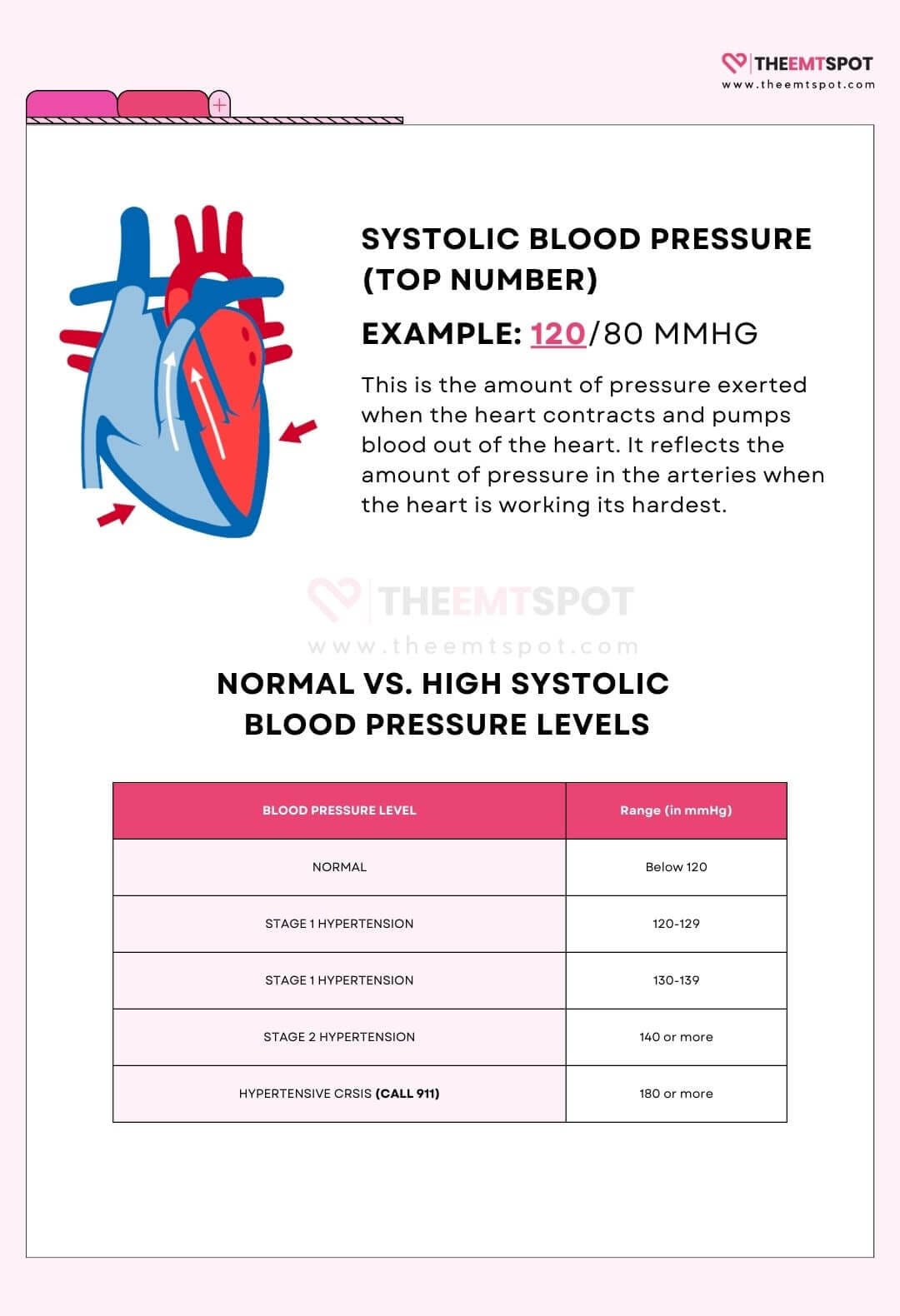
Systolic pressure occurs during systole, the phase when the heart muscle contracts and ejects blood into the aorta and arteries.
Diastolic pressure occurs during diastole, the phase when the heart muscle relaxes and the chambers refill with blood before the next contraction.
| Aspect | Systolic Blood Pressure | Diastolic Blood Pressure |
|---|---|---|
| Definition | Pressure exerted on arterial walls during the contraction of the heart muscle. | Pressure in the arteries when the heart muscle is at rest between beats. |
| Mechanism | Heart contracts during systole, ejecting blood into the arteries. Produces the peak pressure wave in the circulatory system. | Heart relaxes during diastole. Chambers refill with blood. Pressure drops to its lowest point in the cycle. |
| Normal range | Below 120 mmHg | Below 80 mmHg |
| Hypertension threshold | 130 mmHg or above (AHA/ACC 2025) | 80 mmHg or above (AHA/ACC 2025) |
| Position in reading | Top number – e.g. 120/80 mmHg | Bottom number – e.g. 120/80 mmHg |
| Age trend | Rises continuously throughout life as arteries stiffen. | Rises until around age 50, then plateaus or falls as arterial compliance decreases. |
| Primary risk group | Adults over 50 – dominant cardiovascular risk marker in older populations. | Adults under 50 – independently predicts coronary risk in younger and middle-aged adults. |
The gap between the two numbers, known as pulse pressure, reflects the force generated by each heartbeat and serves as an additional indicator of arterial stiffness and vascular health.
For a detailed breakdown of pulse pressure values and their clinical significance, see the pulse pressure guide.
Which is more important: systolic or diastolic blood pressure?
Both numbers independently predict cardiovascular risk, but their relative importance shifts with age.
Flint AC and colleagues published “Effect of Systolic and Diastolic Blood Pressure on Cardiovascular Outcomes” in the New England Journal of Medicine in 2019, analyzing data from 1.3 million adults over eight years.
The study found that systolic hypertension carried a higher hazard ratio for cardiovascular events than diastolic hypertension (1.18 vs 1.06 per z-score unit), but both independently predicted myocardial infarction and stroke.
How does age affect systolic and diastolic blood pressure risk?
Age affects which blood pressure number carries greater cardiovascular risk, with diastolic pressure dominating in younger adults and systolic pressure becoming the primary risk marker after age 50.
In adults under 50, diastolic pressure tends to rise first, and elevated diastolic readings carry meaningful cardiovascular risk even when systolic pressure remains below 130 mmHg.
After age 50, arteries stiffen progressively.
Systolic pressure continues to rise while diastolic pressure often plateaus or falls.
Systolic hypertension becomes the dominant pattern in older adults and carries stronger independent risk for stroke, heart failure, and kidney disease in this age group.
Isolated systolic hypertension (elevated systolic with normal diastolic) represents the most common form of hypertension in adults over 60, occurring in an estimated 12% to 25% of this population depending on the diagnostic threshold applied (Tin LL et al., Journal of Human Hypertension, 2002).
Why do clinicians monitor both systolic and diastolic blood pressure?
Clinicians monitor both values because neither number alone fully captures cardiovascular risk.
A clinician evaluates both readings together, alongside age, comorbidities, and the overall pattern of readings over time.
The 2025 AHA/ACC guidelines define hypertension as systolic pressure at or above 130 mmHg or diastolic pressure at or above 80 mmHg, treating both thresholds as independently actionable.
What is systolic blood pressure?
Systolic blood pressure is the peak pressure in the arteries generated during each heartbeat, recorded as the top number in a blood pressure reading.
A normal systolic reading for most adults falls below 120 mmHg, according to the 2025 AHA/ACC guidelines.
What is low systolic blood pressure?
Low systolic blood pressure is defined as a systolic reading below 90 mmHg and is classified as hypotension when it causes symptoms or impairs organ perfusion.
Wessely S and colleagues, in a 1990 population study published in the British Medical Journal (n=7,383), found that chronic low blood pressure is associated with persistent fatigue, dizziness, and difficulty concentrating, particularly in women under 50.
Common causes of low systolic blood pressure include the following conditions.
Management focuses on identifying and treating the underlying cause.
Common approaches include adjusting medications, increasing fluid and sodium intake where appropriate, and using compression stockings for orthostatic hypotension.
For a detailed guide to low blood pressure types, thresholds, and treatment approaches, see the hypotension guide.
What is high systolic blood pressure?
High systolic blood pressure is defined as a systolic reading of 130 mmHg or above under the 2025 AHA/ACC guidelines, rising to 140 mmHg or above under the 2018 ESC/ESH European guidelines.
Elevated systolic pressure is often called a silent condition because it produces no symptoms while damaging blood vessels, the heart, and the kidneys over years.
Banegas JR and colleagues published a large-scale study in the New England Journal of Medicine in 2018 demonstrating that 24-hour ambulatory systolic pressure is a stronger predictor of all-cause and cardiovascular mortality than office measurements, underscoring the value of home monitoring.
Common causes of high systolic blood pressure are listed below.
Untreated high systolic blood pressure contributes to heart disease, stroke, kidney damage, retinopathy, and cognitive decline.
For a comprehensive overview of treatment targets and evidence-based interventions, see the hypertension guide.
What is isolated systolic hypertension?
Isolated systolic hypertension (ISH) is defined as systolic blood pressure at or above 130 mmHg combined with diastolic blood pressure below 80 mmHg.
Arterial stiffening with age is the primary driver.
The aorta and large arteries lose compliance, amplifying the pressure wave generated with each heartbeat.
Additional causes of ISH include hyperthyroidism, which increases cardiac output; aortic regurgitation, which causes large stroke volumes; and diabetes, which accelerates arterial stiffening through glycation of vessel walls.
ISH is the most common form of hypertension in adults over 60 and carries independent risk for stroke, heart failure, and dementia even before systolic pressure reaches the stage 2 threshold (140 mmHg).
Treatment requires careful titration, because lowering systolic pressure too aggressively can reduce diastolic pressure below 60 mmHg and impair coronary perfusion, which occurs primarily during diastole.
For context on how mean arterial pressure relates to coronary perfusion targets, see the mean arterial pressure guide.
What is diastolic blood pressure?
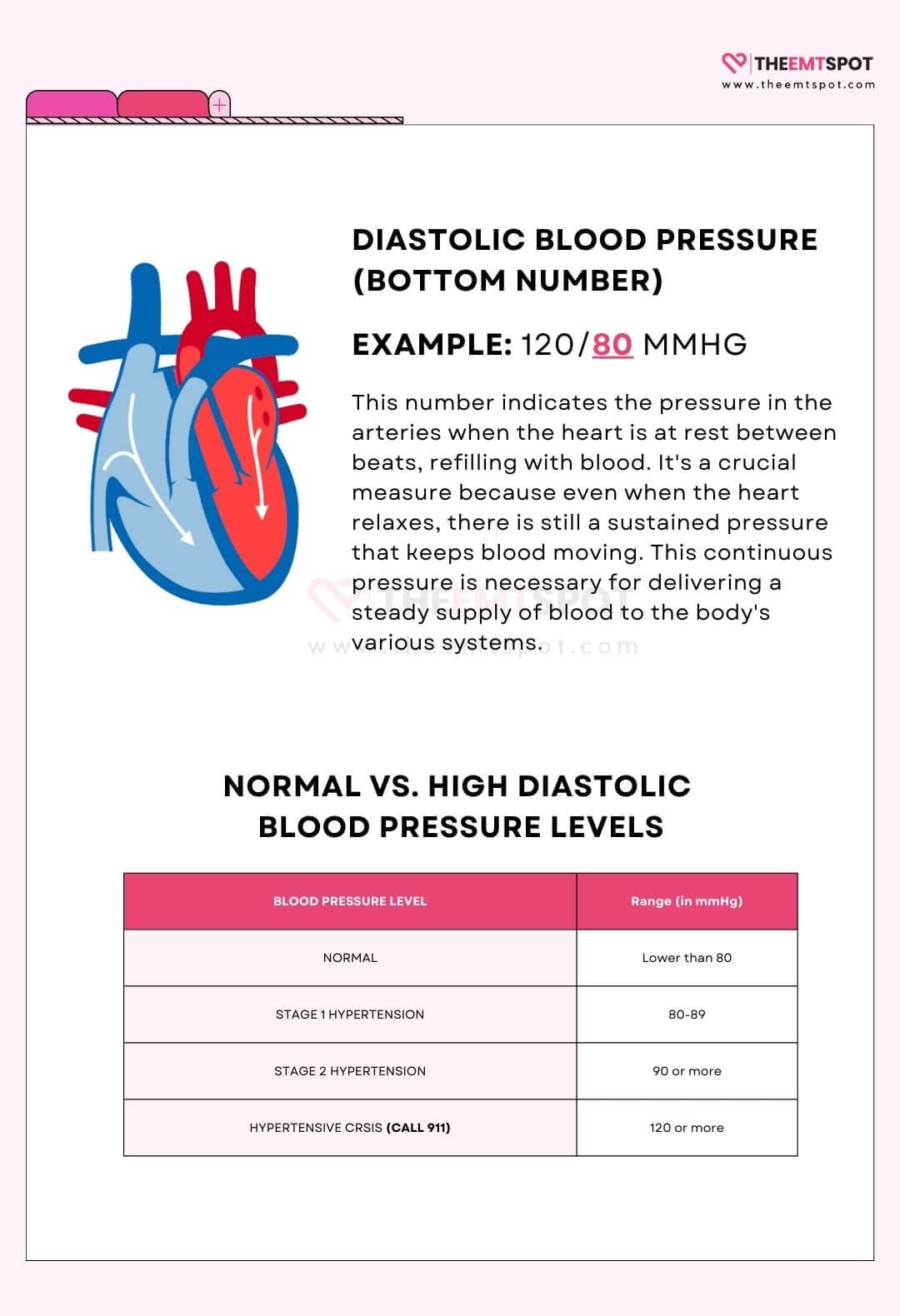
Diastolic blood pressure is the pressure remaining in the arteries during the relaxation phase between heartbeats, recorded as the bottom number in a blood pressure reading.
A normal diastolic reading for most adults falls below 80 mmHg under the 2025 AHA/ACC guidelines.
What is low diastolic blood pressure?
Low diastolic blood pressure is defined as a diastolic reading below 60 mmHg.
Most coronary artery perfusion occurs during diastole, when the heart muscle is relaxed and the coronary vessels are open to blood flow.
A diastolic pressure below 60 mmHg reduces coronary perfusion pressure, increasing the risk of myocardial ischemia, particularly in patients with pre-existing coronary artery disease.
Common causes of low diastolic pressure include the following.
Symptoms of low diastolic pressure include dizziness, fainting, palpitations, fatigue, and poor concentration.
Management involves identifying and correcting the underlying cause, adjusting any medications that may be contributing, and maintaining adequate hydration.
What is high diastolic blood pressure?
High diastolic blood pressure is defined as a diastolic reading of 80 mmHg or above under the 2025 AHA/ACC guidelines, or 90 mmHg or above under the 2018 ESC/ESH European guidelines.
Flint AC and colleagues (NEJM, 2019) found that diastolic hypertension independently predicted myocardial infarction and stroke over eight years, with a hazard ratio of 1.06 per z-score unit, even after accounting for systolic pressure levels.
High diastolic pressure is more common in younger and middle-aged adults and reflects elevated vascular resistance rather than arterial stiffening, which is the primary driver of high systolic pressure in older adults.
Common causes of elevated diastolic pressure include the following conditions.

Persistently high diastolic pressure increases the risk of heart disease, stroke, kidney disease, and arterial damage through sustained mechanical stress on vessel walls.
Management follows the same evidence-based approach as systolic hypertension: sodium reduction, weight loss, aerobic exercise, stress management, and medication when lifestyle changes alone are insufficient.
Routine cardiovascular checkups are recommended for adults in their 40s and older, regardless of which number is elevated.
What is isolated diastolic hypertension?
Isolated diastolic hypertension (IDH) is defined as diastolic blood pressure in the hypertensive range while systolic blood pressure remains below the hypertensive threshold.
Under the 2025 AHA/ACC guidelines, IDH is defined as diastolic pressure at or above 80 mmHg with systolic pressure below 130 mmHg.
IDH is most prevalent in younger and middle-aged adults and reflects elevated peripheral vascular resistance rather than the arterial stiffening that drives isolated systolic hypertension in older populations.
Common causes of IDH include the following.
Evidence on IDH cardiovascular risk is mixed and depends on the diagnostic threshold used.
McEvoy JW and colleagues (JAMA, 2020) found that IDH defined by the 2017 ACC/AHA criteria (diastolic at or above 80 mmHg) was not significantly associated with increased atherosclerotic cardiovascular disease risk in their longitudinal analysis of 8,703 US adults.
A 2021 meta-analysis by Huang and colleagues in Frontiers in Cardiovascular Medicine (489,814 participants, 15 studies) found that IDH defined by older ESC criteria (diastolic at or above 90 mmHg) was associated with increased cardiovascular event risk (HR 1.28) and cardiovascular mortality (HR 1.45), particularly in younger Asian adults.
Current clinical guidance recommends lifestyle intervention for IDH under ACC/AHA thresholds, reserving medication for cases progressing to higher diastolic levels or accompanied by additional cardiovascular risk factors.
Can diastolic blood pressure be too low?
Diastolic blood pressure can be too low – readings below 60 mmHg are associated with increased risk of myocardial ischemia because coronary artery perfusion occurs primarily during diastole, when the heart muscle relaxes.
Reducing diastolic pressure below this threshold during antihypertensive treatment reduces the coronary perfusion pressure available to supply the left ventricular myocardium.
Clinicians treating hypertension typically aim to maintain diastolic pressure above 60 mmHg, particularly in patients with existing coronary artery disease, to balance the benefits of blood pressure reduction against the risk of cardiac under-perfusion.
Symptoms such as chest pain, dizziness, or new-onset fatigue during antihypertensive therapy warrant prompt clinical reassessment to evaluate whether diastolic pressure has fallen too low.
How is high blood pressure diagnosed and treated?
High blood pressure is diagnosed when systolic pressure reaches 130 mmHg or higher, or diastolic pressure reaches 80 mmHg or higher, based on the 2025 AHA/ACC guidelines.
A single elevated office reading is not sufficient for diagnosis.
Confirmation requires multiple readings across separate occasions, typically verified through home blood pressure monitoring (HBPM) or 24-hour ambulatory blood pressure monitoring (ABPM), to rule out white coat hypertension and capture the true out-of-office blood pressure pattern.
What is the blood pressure treatment target for adults with hypertension?
The treatment target for most adults with hypertension is a blood pressure below 130/80 mmHg, to reduce the risk of heart attack, stroke, kidney disease, and heart failure.
Treatment for most patients at the elevated or stage 1 level begins with lifestyle modification before medication is considered.
The four lifestyle interventions with the strongest evidence for reducing both systolic and diastolic pressure are listed below.
For a complete implementation guide covering each intervention, see the how to lower blood pressure guide and the blood pressure diet guide.
What medications are used to lower systolic and diastolic blood pressure?
Five major antihypertensive drug classes are used to lower blood pressure, each reducing both systolic and diastolic readings through a different mechanism.
Medication is added when lifestyle changes do not achieve the target blood pressure within 3 to 6 months, or when cardiovascular risk is high at presentation.
Individual responses to antihypertensive medications vary, and some medications prescribed for other conditions can raise or lower blood pressure as a side effect, requiring close monitoring and periodic adjustment.
Why does blood pressure consistency between visits matter for cardiovascular outcomes?
Blood pressure consistency between visits matters because a single target reading at a clinic visit does not fully protect against cardiovascular events if readings fluctuate widely between sessions.
Fatani N, Buckley LF, and colleagues published a post-hoc analysis of the SPRINT trial in JACC (2021), demonstrating that greater time in systolic blood pressure target range (Time in Target Range, TTR) independently predicted lower rates of major adverse cardiovascular events, even after adjusting for mean blood pressure.
Regular home monitoring, consistent medication adherence, and routine follow-up appointments together maximize the proportion of time that both systolic and diastolic pressures remain within healthy limits.
How do you take blood pressure accurately at home?
To take blood pressure accurately at home, use a validated upper-arm cuff monitor, sit in the correct position, rest for five minutes beforehand, and follow a consistent two-reading protocol.
Wrist cuffs and cuffless wearable devices remain unvalidated for clinical decision-making.
For a full guide to cuff sizing, monitor selection, and measurement timing, see the how to take blood pressure guide.
How do you improve blood pressure reading accuracy at home?
What time of day should you take blood pressure?
Morning and evening are the two recommended measurement windows under the 2025 AHA/ACC home monitoring protocol.
| Time / Scenario | Guidance |
|---|---|
| Morning (upon waking) | Measure before taking any medication and before eating or drinking caffeine. Morning readings reflect baseline pressure unaffected by daily activity and are typically the highest readings of the day. |
| Evening (before dinner) | Measure before eating and before alcohol intake. Evening readings capture pressure after a full day of activity and serve as a second data point for tracking daily variation. |
| Consistent timing each day | Taking readings at the same times every day ensures readings are comparable across days and reduces variation caused by activity or diet differences. |
| Before medication (morning) | Measuring before the morning dose captures the trough pressure point, which shows whether medication is maintaining adequate control through the dosing interval. |
| For 7 consecutive days minimum | The 2025 AHA/ACC and ESH guidelines recommend at least 7 days of paired morning and evening readings. Discard the first day. Average the remaining 12 readings to obtain a representative home blood pressure value. |
| Multiple times per day (if advised) | A clinician may request more frequent monitoring during medication adjustment, at the start of treatment, or when readings are inconsistent. Follow the specific schedule provided. |
What do the blood pressure numbers mean on the AHA chart?
The AHA blood pressure chart classifies readings into five categories based on both the systolic and diastolic number.
The higher of the two numbers determines the classification.
Blood Pressure Categories
AHA 2023 guidelines. Click any row to expand.
| Category | Systolic | Diastolic | Recommended action |
|---|---|---|---|
| Severe hypotensionDangerously low | < 70 mmHg |
< 40 mmHg |
Seek emergency care immediately ⌄ |
| HypotensionLow blood pressure | 70 – 89 mmHg |
40 – 59 mmHg |
Consult a doctor if symptomatic ⌄ |
| NormalHealthy range | < 120 mmHg |
< 80 mmHg |
Maintain healthy lifestyle ⌄ |
| ElevatedPre-hypertension risk | 120 – 129 mmHg |
< 80 mmHg |
Lifestyle changes recommended ⌄ |
| Stage 1 hypertensionHigh blood pressure | 130 – 139 mmHg |
80 – 89 mmHg |
Doctor consultation advised ⌄ |
| Stage 2 hypertensionHigh blood pressure | ≥ 140 mmHg |
≥ 90 mmHg |
Medical treatment required ⌄ |
| Hypertensive crisisEmergency | ≥ 180 mmHg |
≥ 120 mmHg |
Call emergency services now ⌄ |
A reading of 132/72 mmHg falls into the Stage 1 Hypertension category because the systolic value crosses the 130 mmHg threshold, even though the diastolic value is within the normal range.
For the complete classification table with thresholds for each category and guidance on when to seek medical care, see the blood pressure readings guide.
More in this topic