High blood pressure, or hypertension, is a condition in which the force of blood against arterial walls remains persistently elevated, increasing the risk of heart attack, stroke, and kidney damage over time.
Blood pressure is expressed as two numbers in millimeters of mercury (mmHg).
The systolic number (top) measures pressure during each heartbeat.
The diastolic number (bottom) measures pressure between beats.
According to the 2025 American Heart Association and American College of Cardiology (AHA/ACC) guidelines, hypertension is defined as a systolic reading of 130 mmHg or above, or a diastolic reading of 80 mmHg or above, measured on two or more separate occasions.
Hypertension affects approximately 1.28 billion adults worldwide, according to the World Health Organization (2023), making it the leading modifiable risk factor for cardiovascular disease globally.
Most people with hypertension have no symptoms.
The condition is identified through regular blood pressure measurement, not through self-reported signs.
What are the types of high blood pressure (hypertension)?
Hypertension is classified into three broad categories: systemic (by origin and mechanism), local (by affected vascular bed), and categorical (by clinical severity).
Systemic hypertension
Systemic hypertension occurs when sustained elevated pressure develops in the arteries that carry blood away from the heart.
Essential (primary) hypertension
Essential hypertension has no identifiable secondary cause and accounts for approximately 85 to 95% of all hypertension cases in adults.
Essential hypertension develops gradually through the interaction of genetic predisposition, age, and modifiable lifestyle factors.
Secondary hypertension
Secondary hypertension is caused by an identifiable underlying condition, most commonly chronic kidney disease, primary aldosteronism, obstructive sleep apnea, or thyroid dysfunction.
Secondary hypertension accounts for 5 to 15% of hypertension cases and often presents with more severe or treatment-resistant readings.
Treating the underlying cause frequently normalizes or substantially reduces blood pressure.
Isolated systolic hypertension (ISH)
Isolated systolic hypertension is defined as systolic blood pressure at or above 130 mmHg with diastolic pressure below 80 mmHg.
Isolated systolic hypertension is the most common form of hypertension in adults over 60, affecting more than 65% of hypertensive patients in this age group, and results primarily from age-related arterial stiffening.
Resistant hypertension
Resistant hypertension is blood pressure that remains at or above 130/80 mmHg despite concurrent use of three or more antihypertensive medications of different classes at optimal doses, including a diuretic.
Spironolactone, a mineralocorticoid receptor antagonist, has shown the strongest evidence for add-on blood pressure reduction in resistant cases (Williams B et al., The Lancet, 2015).
Masked hypertension
Masked hypertension describes readings that are normal in a clinical setting but elevated in daily life.
Under the 2025 AHA/ACC definition, office blood pressure below 130/80 mmHg combined with average awake ambulatory or home blood pressure at or above 130/80 mmHg constitutes masked hypertension.
Masked hypertension carries the same cardiovascular risk as sustained hypertension and requires home or ambulatory monitoring to identify.
White coat hypertension
White coat hypertension produces elevated readings in clinical settings but normal readings outside them.
Up to 30% of patients show this pattern (Mancia et al., Journal of Hypertension, 2019).
Ambulatory blood pressure monitoring over 24 hours is the most reliable method to distinguish white coat hypertension from true sustained hypertension.
Nocturnal hypertension
Nocturnal hypertension is defined as average nighttime blood pressure at or above 120/70 mmHg on 24-hour ambulatory monitoring.
Each 10 mmHg increase in nighttime systolic pressure is independently associated with a higher risk of cardiovascular events, including stroke, beyond what daytime readings predict.
Postpartum hypertension
Postpartum hypertension is blood pressure at or above 140/90 mmHg occurring after delivery, typically within the first six weeks.
Postpartum hypertension affects approximately 2% of pregnancies and requires close monitoring due to the risk of postpartum preeclampsia and stroke.
Preeclampsia (gestational hypertension)
Preeclampsia is characterized by new-onset hypertension at or above 140/90 mmHg after 20 weeks of gestation, accompanied by proteinuria or signs of end-organ damage.
Its global prevalence is approximately 4.6% across high- and low-income countries (Mayrink et al., Scientific World Journal, 2018), and it is a leading cause of maternal and perinatal morbidity.
Local hypertension
Local hypertension refers to elevated pressure within a specific vascular bed rather than the systemic arterial system.
Severity index
The 2025 AHA/ACC guidelines classify blood pressure into the following categories based on severity.
Elevated blood pressure: systolic 120 to 129 mmHg with diastolic below 80 mmHg.
No medication is indicated at this stage; lifestyle modification is the recommended first step.
For a full explanation of elevated blood pressure readings and what they mean clinically, see the elevated blood pressure guide.
Stage 1 hypertension: systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg.
Lifestyle intervention is the primary treatment, with medication added when the 10-year cardiovascular risk is 10% or higher.
For a detailed guide on Stage 1 readings and their management, see the Stage 1 hypertension guide.
Stage 2 hypertension: systolic 140 mmHg or above or diastolic 90 mmHg or above.
Medication is indicated alongside lifestyle modification at this stage.
For a detailed guide on Stage 2 readings and treatment thresholds, see the Stage 2 hypertension guide.
Hypertensive crisis: systolic at or above 180 mmHg and/or diastolic at or above 120 mmHg.
Readings at this level require immediate clinical evaluation to determine whether end-organ damage is present.
See the hypertensive crisis guide for emergency management.
What are the symptoms and signs of high blood pressure (hypertension)?
Hypertension is almost always asymptomatic.
The American Heart Association, Mayo Clinic, and the 2025 AHA/ACC guidelines all confirm that most people with even significantly elevated blood pressure feel entirely normal, which is why the condition is described as a silent killer.
The only reliable way to identify hypertension is through accurate, repeated blood pressure measurement, not through self-reported symptoms.
A small number of people with severely elevated blood pressure, particularly readings at or above 180/120 mmHg (hypertensive crisis), may experience symptoms that reflect acute end-organ stress.
Severe headache
Particularly at the back of the head on waking, associated with hypertensive urgency or emergency rather than routine hypertension.
Visual disturbances
Including blurred vision or transient vision loss, reflecting hypertensive retinopathy or raised intracranial pressure.
Chest pain or shortness of breath
Indicating possible hypertensive cardiac involvement.
Neurological changes
Including confusion or difficulty speaking, associated with hypertensive encephalopathy or stroke.
Nausea and vomiting
In the context of severely elevated readings and raised intracranial pressure.
Nosebleeds, dizziness, facial flushing, and palpitations are commonly attributed to hypertension in popular sources but are not established clinical indicators of the condition.
These symptoms are not reliably associated with blood pressure level and have other more common causes.
Attributing such symptoms to hypertension without measurement can provide false reassurance or prompt unnecessary alarm.
Any reading at or above 180/120 mmHg accompanied by any of the acute symptoms listed above requires immediate emergency assessment.
Call emergency services rather than waiting to see whether symptoms resolve.
What are the risk factors and causes of high blood pressure (hypertension)?
Hypertension develops from the interaction of non-modifiable genetic and biological factors with modifiable lifestyle and environmental contributors.
Non-modifiable risk factors
Genetics and family history
Genetic predisposition accounts for approximately 30 to 50% of blood pressure variability across individuals (Williams B et al., Journal of Hypertension, 2018).
Having one hypertensive parent approximately doubles the lifetime risk of developing hypertension, with risk rising further when both parents are affected.
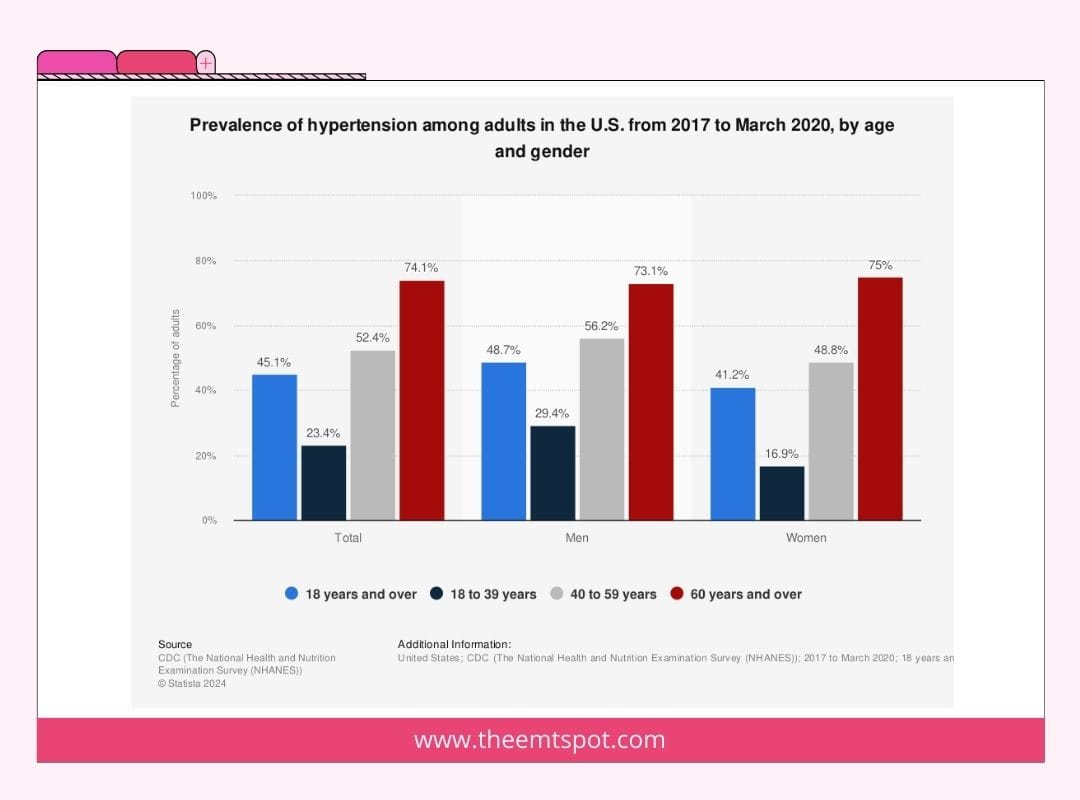
Age
Systolic blood pressure rises continuously throughout adult life as arterial walls lose elasticity.
Diastolic pressure rises until approximately age 50, then plateaus or falls as arterial compliance decreases.
By age 60, the majority of adults in high-income countries meet the criteria for hypertension under the 2025 AHA/ACC definition.
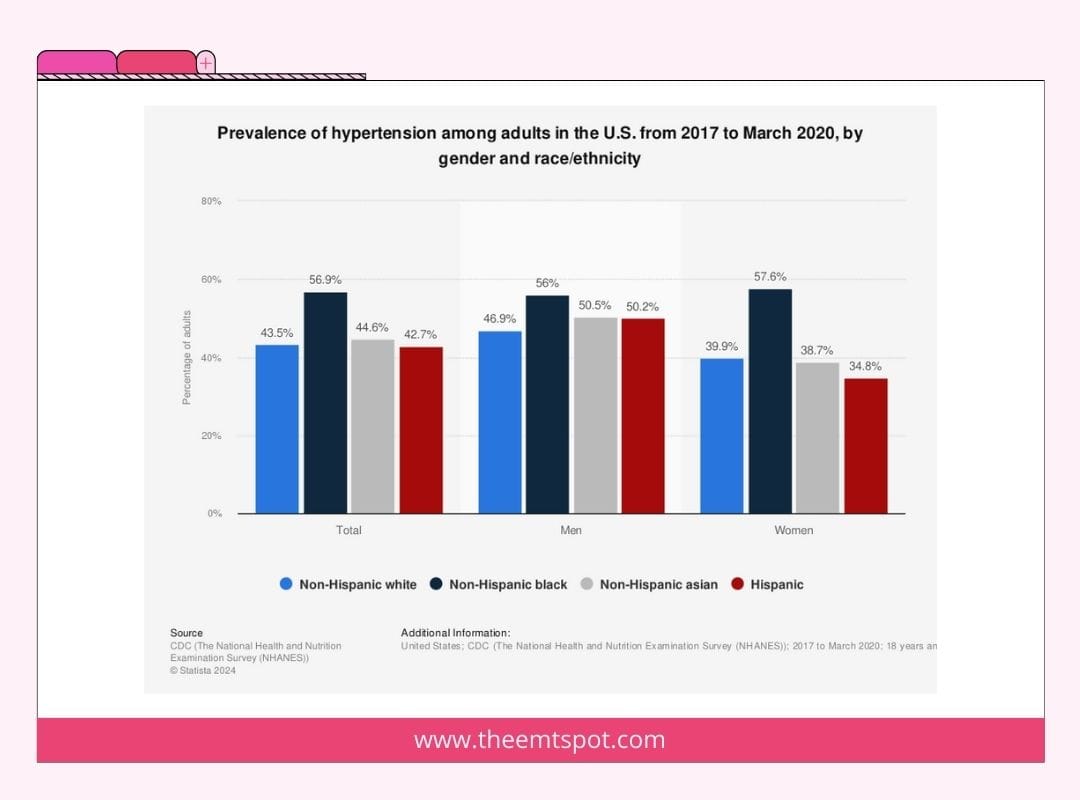
Ethnicity
Black adults develop hypertension at higher rates, at younger ages, and with greater severity than other ethnic groups.
Hypertension prevalence among Black adults in the United States reaches approximately 56%, compared to 48% among White adults (AHA Heart Disease and Stroke Statistics, 2023).
The mechanisms include a higher prevalence of salt sensitivity and greater activation of the renin-angiotensin-aldosterone system in response to high sodium intake.
Modifiable lifestyle risk factors
High sodium intake
Excess dietary sodium promotes fluid retention and raises systemic vascular resistance.
Reducing sodium intake by 1,000 mg per day produces a systolic reduction of approximately 5 to 6 mmHg in hypertensive individuals (He FJ et al., BMJ, 2013).
The effect is largest in individuals who are salt-sensitive, older, or of Black ethnicity.
Insufficient potassium intake amplifies the blood pressure effect of high sodium, as potassium directly counterbalances sodium in renal handling.
Physical inactivity
Regular aerobic exercise reduces systolic blood pressure by an average of 5 to 8 mmHg, making physical inactivity one of the most directly reversible contributors to hypertension (Cornelissen VA and Smart NA, Journal of the American Heart Association, 2013).
At least 150 minutes of moderate-intensity aerobic activity per week is recommended by the AHA as a primary intervention for elevated and stage 1 hypertension.
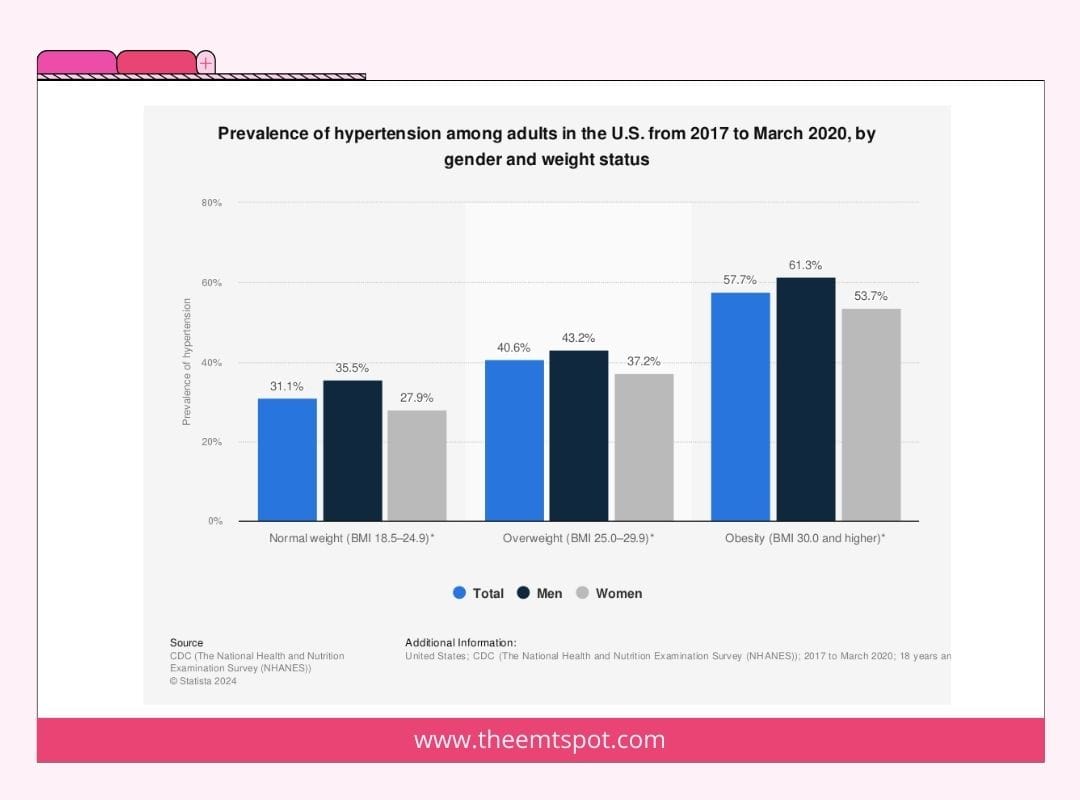
Obesity
Each 5 kg increase in body weight is associated with an approximately 2 to 3 mmHg rise in systolic blood pressure (Neter JE et al., Hypertension, 2003).
Obesity activates the sympathetic nervous system, the renin-angiotensin-aldosterone system, and promotes sodium retention, all of which raise blood pressure independently.
Weight loss of 5 to 10 kg in overweight or obese hypertensive patients produces clinically meaningful reductions in both systolic and diastolic pressure.
Alcohol
Each additional standard drink per day above moderate consumption raises systolic blood pressure by approximately 1 mmHg (Roerecke M et al., Lancet Public Health, 2017).
Chronic heavy alcohol use is among the most common reversible causes of secondary hypertension.
Limiting intake to no more than one drink per day for women and two for men is endorsed by the 2025 AHA/ACC guidelines.
Tobacco
Each cigarette produces an acute rise in blood pressure of approximately 5 to 10 mmHg lasting 20 to 30 minutes, driven by nicotine-mediated sympathetic activation.
Long-term smoking accelerates arterial stiffening through oxidative damage to endothelial cells, sustaining chronically elevated vascular resistance.
Cessation improves endothelial function measurably within weeks of stopping.
Poor sleep and sleep apnea
Sleeping fewer than 6 hours per night raises the hazard ratio for incident hypertension by approximately 1.07, with women showing notably higher vulnerability than men (Hosseini et al., PLOS ONE, 2024).
Obstructive sleep apnea (OSA) produces repeated overnight oxygen drops that trigger cortisol and adrenaline release, producing elevated morning blood pressure readings.
Treating OSA with CPAP reduces systolic blood pressure by an average of 2 to 3 mmHg (Bratton DJ et al., European Respiratory Journal, 2014).
Chronic stress
Chronic psychological stress activates the sympathetic nervous system, raising heart rate and vascular resistance.
People with anxiety or depression show measurable cardiovascular risk factor changes up to six months earlier than those without these conditions, suggesting stress is an early driver rather than a late consequence (Civieri G et al., JACC: Advances, 2024).
Caffeine
Caffeine produces a temporary spike in blood pressure of 3 to 15 mmHg, most pronounced in individuals who do not consume it regularly.
Long-term habitual caffeine intake at moderate levels is not consistently associated with sustained hypertension in most population studies.
Hypertensive patients who are caffeine-sensitive may benefit from reducing intake, but this is not universally recommended.
Medical conditions that cause or worsen hypertension
Chronic kidney disease
Chronic kidney disease (CKD) impairs sodium and fluid excretion, activates the renin-angiotensin-aldosterone system, and promotes oxidative stress in blood vessels, all of which raise blood pressure.
Hypertension and CKD form a bidirectional relationship in which each condition worsens the other over time.
Controlling blood pressure is the primary intervention to slow CKD progression.
Diabetes
Insulin resistance impairs endothelial function, increases sodium retention, and activates the sympathetic nervous system, all of which raise blood pressure.
Hypertension affects approximately 75% of adults with type 2 diabetes and shares common risk factors, including obesity and physical inactivity.
The combination multiplies cardiovascular risk beyond either condition alone.
High cholesterol
Elevated LDL cholesterol promotes atherosclerosis, narrowing and stiffening arteries and raising systemic vascular resistance.
Hypertension and hypercholesterolemia frequently coexist and share the same dietary and lifestyle drivers.
Managing both simultaneously is endorsed by the AHA Life’s Essential 8 framework (2022) as the most effective approach to reducing cardiovascular event risk.
Hormonal and endocrine disorders
Primary aldosteronism, the most common endocrine cause of secondary hypertension, affects an estimated 5 to 10% of all hypertensive patients.
Cushing’s syndrome, pheochromocytoma, and thyroid dysfunction (both hypo- and hyperthyroidism) each raise blood pressure through distinct hormonal mechanisms.
Identifying and treating these conditions frequently normalizes blood pressure without long-term antihypertensive therapy.
Medications and dietary supplements
Several common medication classes raise blood pressure through distinct mechanisms.
Supplements containing ephedra, licorice root, or high-dose ginseng can also elevate blood pressure.
A full medication and supplement review is recommended whenever hypertension is unexplained or newly treatment-resistant.
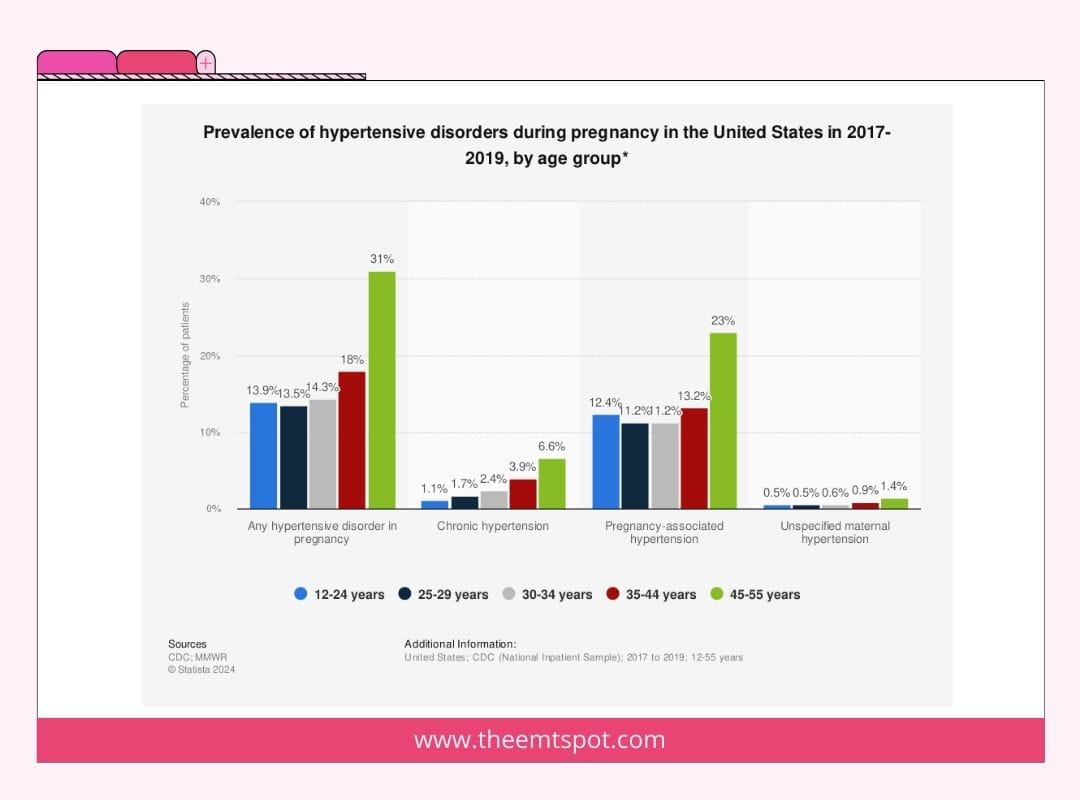
Pregnancy (gestational hypertension)
Gestational hypertension develops after 20 weeks of gestation and typically resolves within 12 weeks postpartum.
Gestational hypertension is distinct from preeclampsia, which involves end-organ damage or proteinuria in addition to elevated blood pressure.
Women with gestational hypertension have a significantly higher lifetime risk of developing chronic hypertension and cardiovascular disease compared to women with normotensive pregnancies.
What do MAP and Pulse Pressure tell you in hypertension?
Mean arterial pressure (MAP) and pulse pressure (PP) provide additional clinical context beyond systolic and diastolic readings alone.
MAP represents the average driving pressure throughout the cardiac cycle and is calculated as (Systolic + 2 x Diastolic) / 3.
Normal MAP falls between 70 and 100 mmHg.
A MAP above 100 mmHg sustained over time damages arterial walls and increases the risk of stroke, kidney disease, and left ventricular hypertrophy.
For a full explanation of MAP thresholds, see the mean arterial pressure guide.
Pulse pressure (PP) is the difference between systolic and diastolic pressure and reflects arterial stiffness.
Normal PP falls between 40 and 60 mmHg.
A widened pulse pressure above 60 mmHg is common in isolated systolic hypertension and is an independent predictor of cardiovascular events in adults over 50, beyond what systolic pressure alone predicts.
For a full breakdown of pulse pressure values, see the pulse pressure guide.
What are the diagnosis and tests for high blood pressure (hypertension)?
Diagnosing hypertension requires confirmation across multiple readings, not a single elevated measurement.
The 2025 AHA/ACC guidelines specify that hypertension diagnosis requires readings at or above 130/80 mmHg on at least two separate occasions.
Blood pressure measurement
Physical examination
A thorough physical examination assesses for signs of end-organ damage and secondary causes of hypertension.
The examination includes auscultation for bruits over the renal arteries (suggesting renovascular disease), fundoscopic examination for hypertensive retinopathy, cardiac auscultation for signs of left ventricular hypertrophy, and assessment of peripheral pulses and edema.
Laboratory tests
Imaging tests
Cardiovascular risk assessment
Diagnosis alone does not determine treatment.
The 2025 AHA/ACC guidelines recommend calculating the 10-year atherosclerotic cardiovascular disease (ASCVD) risk score for all patients with blood pressure in the stage 1 range (130-139/80-89 mmHg).
Medication is indicated when the 10-year ASCVD risk reaches 10% or higher, or when stage 2 readings are confirmed.
What are the treatments for high blood pressure (hypertension)?
Treatment for hypertension targets a blood pressure below 130/80 mmHg for most adults, according to the 2025 AHA/ACC guidelines.
The approach combines lifestyle modification with medication, with the balance determined by blood pressure stage and cardiovascular risk.
What lifestyle changes reduce blood pressure?
Lifestyle modification is the first-line treatment for elevated blood pressure and stage 1 hypertension without high cardiovascular risk.
The following interventions have the strongest clinical evidence.
For a detailed guide on each intervention with implementation steps and dosing evidence, see the how to lower blood pressure guide.
The blood pressure diet guide covers DASH meal planning, sodium targets, and potassium-rich food lists in full detail.
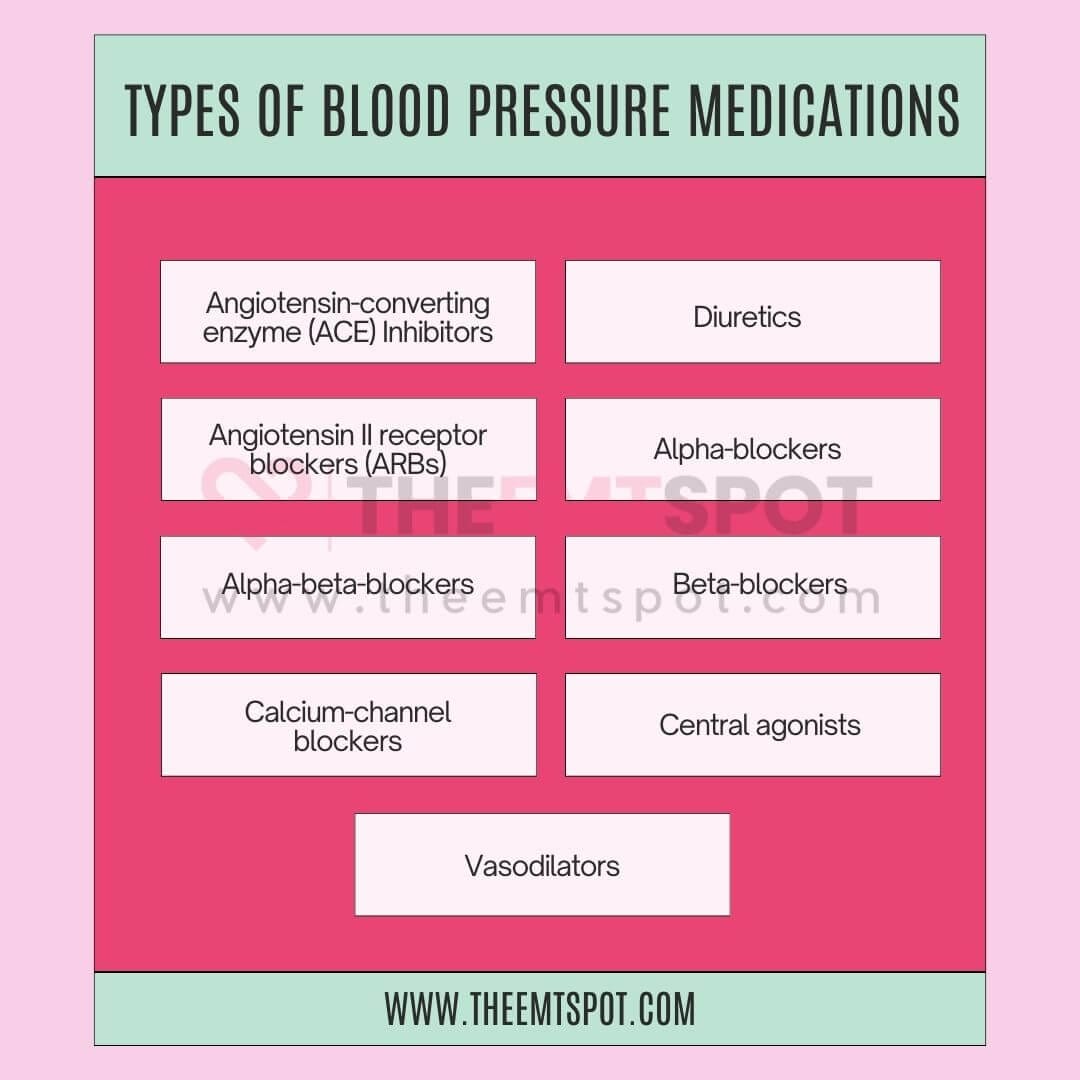
What medications are used to treat high blood pressure (hypertension)?
Medication is added when lifestyle changes do not achieve the target blood pressure within 3 to 6 months, when stage 2 readings are confirmed, or when cardiovascular risk is high at presentation.
Five major antihypertensive drug classes are used, each reducing blood pressure through a different mechanism.
For a full overview of blood pressure medications, their indications, and side effects, see the blood pressure medications guide.
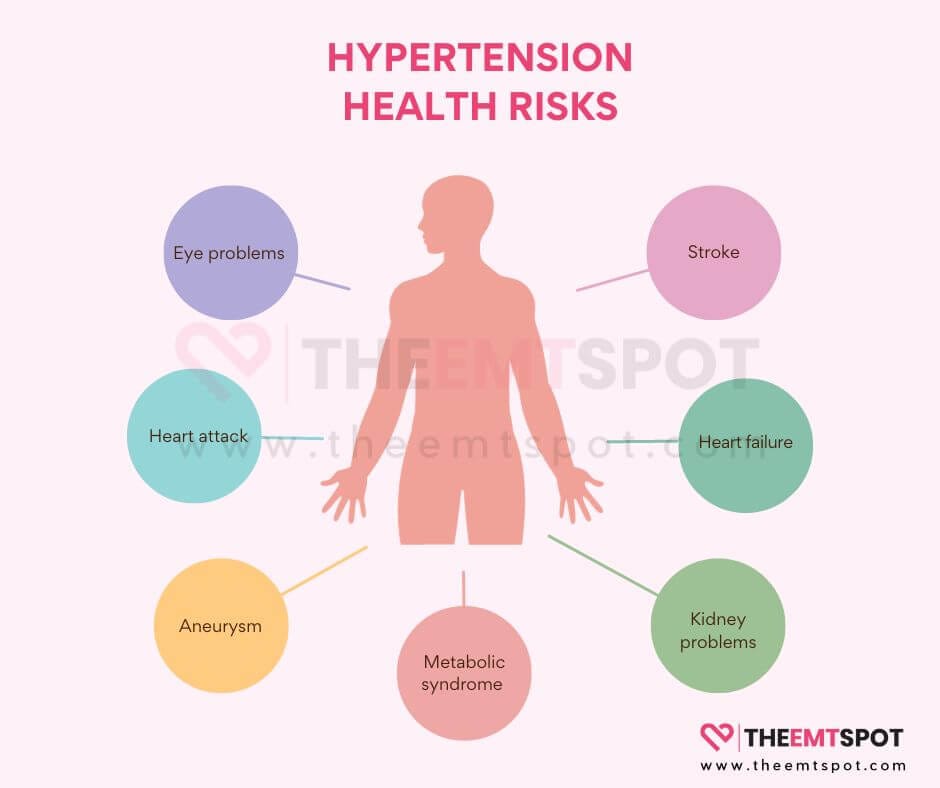
What problems does high blood pressure (hypertension) cause?
Sustained hypertension causes progressive, subclinical damage to blood vessels, the heart, the kidneys, and the brain that produces no symptoms until a serious clinical event occurs.
Heart attack
Hypertension accelerates atherosclerosis in the coronary arteries, increasing plaque formation, arterial narrowing, and the risk of acute plaque rupture triggering a myocardial infarction.
Stroke
Hypertension is the single largest modifiable risk factor for stroke, both ischemic and hemorrhagic. Every 5 mmHg reduction in systolic blood pressure reduces the risk of major cardiovascular events by approximately 10% (Rahimi K et al., The Lancet, 2021).
Heart failure
The heart must pump against chronically elevated resistance, causing the left ventricular muscle to thicken (left ventricular hypertrophy). Over time, this reduces cardiac efficiency and progresses to heart failure with preserved ejection fraction (HFpEF).
Chronic kidney disease
Sustained high pressure damages the glomerular capillaries, reducing filtration capacity and accelerating kidney function decline. Hypertension is the second leading cause of end-stage renal disease after diabetes.
Hypertensive retinopathy
Elevated pressure damages the small blood vessels in the retina, producing changes visible on fundoscopic examination and, in severe cases, leading to vision loss.
Aortic aneurysm
Chronic pressure elevation weakens the aortic wall, increasing the risk of aneurysm formation and, in severe cases, dissection or rupture.
Cognitive decline and dementia
Hypertension during midlife is an independent risk factor for vascular dementia and Alzheimer’s disease. The 2024 Lancet Commission estimates that controlling elevated blood pressure reduces dementia risk by approximately 15% (Livingston G et al., The Lancet, 2024).
How does hypertension affect the heart over time?
The heart responds to chronically elevated vascular resistance by increasing the force of each contraction, causing the left ventricular wall to thicken, a process called left ventricular hypertrophy (LVH).
LVH reduces the heart’s filling capacity, impairs diastolic function, and increases the risk of arrhythmias, including atrial fibrillation.
As hypertension persists without treatment, the coronary arteries that supply the heart become damaged and narrowed, increasing the risk of coronary artery disease, angina, and myocardial infarction.
The combination of LVH and coronary disease is the dominant pathway from hypertension to heart failure.
Does high blood pressure influence cognitive health?
Observational research consistently links midlife hypertension to a higher risk of cognitive decline in later years.
Uncontrolled hypertension damages small blood vessels throughout the brain, producing microinfarcts, white matter lesions, and progressive cortical atrophy.
These changes accumulate over decades before any measurable cognitive symptoms appear.
Hypertension is also associated with an increased risk of cerebral small vessel disease, the vascular cause of approximately 20% of all strokes and a major contributor to vascular dementia.
The 2024 Lancet Commission on Dementia Prevention identified hypertension control as one of the highest-impact interventions available for dementia prevention, with an estimated 15% risk reduction.
What are the challenges in managing hypertension in elderly individuals?
Elderly patients with hypertension frequently have multiple coexisting conditions, polypharmacy, and age-related changes in vascular regulation that complicate management.
The risk of orthostatic hypotension and falls from aggressive pressure reduction requires careful dose titration in older patients, particularly those on multiple antihypertensive agents.
Orthostatic hypotension is defined as a drop in systolic blood pressure of at least 20 mmHg within three minutes of standing and is one of the primary fall risks from antihypertensive treatment in elderly patients.
For a full overview of low blood pressure thresholds and management considerations, see the hypotension guide.
White coat hypertension and masked hypertension are both more prevalent in elderly patients than in younger adults, making ambulatory and home monitoring especially important for accurate diagnosis in this group.
Certain antihypertensive classes, including some beta-blockers and centrally acting agents, carry a higher risk of cognitive side effects in older adults, requiring the cardiovascular benefit to be weighed against this risk for each patient.
The SPRINT trial (Wright JT et al., New England Journal of Medicine, 2015) found that in adults aged 75 and older, intensive blood pressure control targeting below 120 mmHg systolic reduced major cardiovascular events by 25% and all-cause mortality by 27% compared to a standard target of below 140 mmHg.
Treatment decisions must balance this cardiovascular benefit against individual frailty, functional status, and fall risk.
How to prevent hypertension?
Preventing hypertension means sustaining the lifestyle habits that prevent the gradual upward shift in blood pressure that occurs with aging, weight gain, and behavioral changes.
The following strategies have documented evidence for reducing the incidence of hypertension, based on the 2025 AHA/ACC guidelines and established lifestyle intervention data.
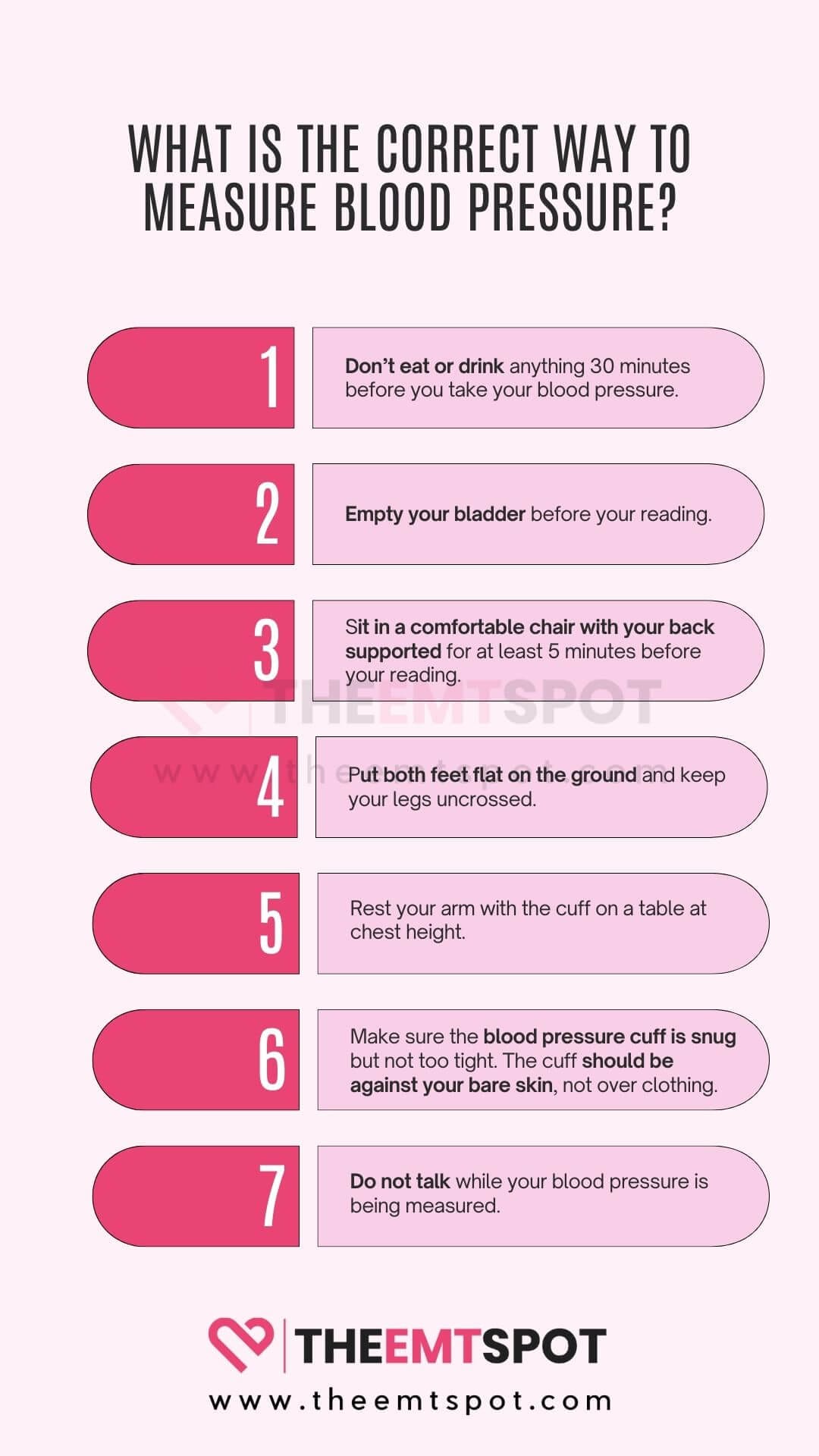
How to take blood pressure at home?
To take blood pressure accurately at home, use a validated upper-arm cuff monitor and follow a consistent protocol.
The 2025 AHA/ACC guidelines and ESH 2023 guidelines both recommend the following approach.
For a step-by-step guide on correct measurement technique, cuff sizing, and timing, see the how to take blood pressure guide.
The best blood pressure monitors guide covers validated upper-arm devices, wrist cuff limitations, and selection criteria for home monitoring.
More in this topic