Preeclampsia is a hypertensive disorder of pregnancy, occurring in 2–8% of pregnancies worldwide and representing one of the leading causes of maternal and fetal morbidity and mortality (American College of Cardiology).
Preeclampsia typically develops after 20 weeks of gestation and is characterized by new-onset hypertension, proteinuria, and potential damage to multiple organs.
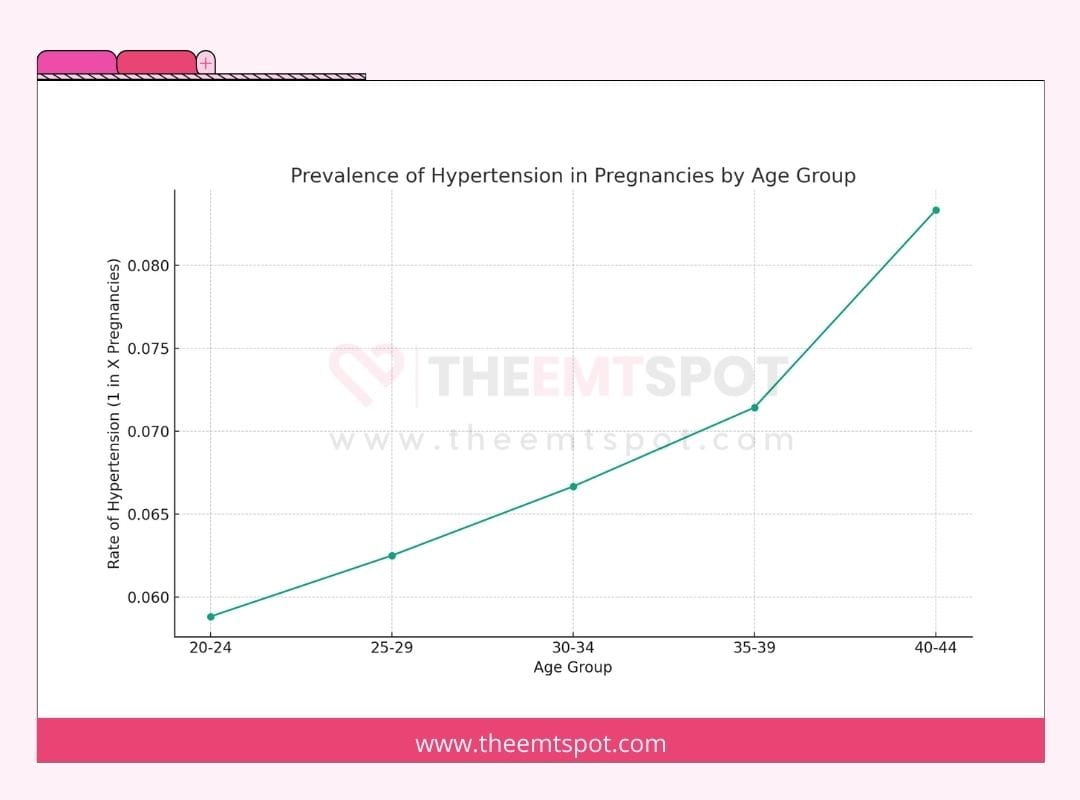
The Centers for Disease Control and Prevention (CDC) highlights that high blood pressure, or hypertension, is prevalent in the United States, occurring in 1 in every 12 to 17 pregnancies among women ages 20 to 44.
Apart from preeclampsia, other forms of high blood pressure during pregnancy include the following.
Preeclampsia involves high blood pressure and potential organ damage, whereas eclampsia represents a more severe progression defined by seizures, which can be life-threatening for both mother and baby.
Preeclampsia is categorized into two forms: one without severe features, managed with close monitoring, and one with severe features, requiring immediate medical intervention.
Preeclampsia typically develops after the 20th week of pregnancy and affects approximately 1 in 25 pregnancies in the United States.
A standard blood pressure chart during pregnancy shows varying normal ranges depending on the stage of pregnancy.
For instance, in the first trimester, the normal systolic blood pressure range is usually below 120 mmHg and diastolic below 80 mmHg. These ranges can slightly change as pregnancy progresses.
One main symptom of preeclampsia is high blood pressure. This is a critical sign for diagnosis and is typically accompanied by protein in the urine, although the latter might not always be present.
The primary cause and risk factor for preeclampsia is not fully understood, but it’s believed to be related to issues with the placenta.
Risk factors include a history of preeclampsia, first-time pregnancy, pre-existing conditions like hypertension or diabetes, obesity, and advanced maternal age.
Genetic factors and immune system responses contribute to risk as well.
Diagnosis typically involves checking blood pressure and assessing for signs like renal dysfunction.
The primary treatment method is delivery, especially in severe cases, with low-dose aspirin recommended for prevention in high-risk women.
One main danger of preeclampsia is the increased risk of cardiovascular and cerebrovascular complications, such as stroke or heart failure.
A significant prevention method involves lifestyle adjustments and possibly low-dose aspirin for those at high risk.
What are the types of preeclampsia?
Preeclampsia, a complication of pregnancy, manifests in two primary forms: mild and severe. Understanding these types is crucial for effective management and treatment.
Mild preeclampsia
- Mild preeclampsia is a less severe form of preeclampsia, a pregnancy-related condition characterized by elevated blood pressure and often accompanied by the presence of protein in the urine.
- In mild preeclampsia, symptoms are less pronounced and may include moderately elevated blood pressure levels and minimal proteinuria.
- This form typically allows for closer monitoring and the possibility of extending the pregnancy, delaying delivery to a safer time for the baby as long as the mother’s condition remains stable without signs of severe features or complications.
- Research consistently shows that Black women face approximately twice the risk of preeclampsia compared to white women, and women of South Asian origin face a 1.5-fold higher risk of preterm preeclampsia, according to a systematic review and meta-analysis published in BJOG (2022).
Severe preeclampsia
- Severe preeclampsia is an advanced form of preeclampsia, a pregnancy complication characterized by significantly elevated blood pressure and often more pronounced protein in the urine.
- Unlike mild preeclampsia, severe preeclampsia presents with more intense symptoms and greater risks, necessitating closer medical monitoring and often earlier intervention, including potentially earlier delivery.
- A 2023 study by researchers from Western University (Canada) and Brown University (USA), published in Nature Communications, identified a toxic protein, cis P-tau, in the blood and placenta of preeclampsia patients, describing it as a central circulating driver of the condition.
- The research identifies cis P-tau as a potential early diagnostic biomarker and therapeutic target, marking a significant advancement in understanding the root cause of severe preeclampsia.
What is the difference between mild and severe preeclampsia?
The transition from mild to severe preeclampsia can be rapid and is marked by an escalation in symptoms and organ damage.
Mild preeclampsia may be managed with close monitoring, whereas preeclampsia with severe features necessitates immediate medical intervention to protect both mother and baby.
Recognizing the transition from preeclampsia to severe features requires vigilant health monitoring throughout pregnancy.
| Aspect | Mild Preeclampsia | Severe Preeclampsia |
|---|---|---|
| Blood Pressure | Elevated, but less than 160/110 mmHg | 160/110 mmHg or higher (Hypertensive emergency) |
| Protein in urine | Present | Present, often in higher amounts |
| Symptoms | Often no noticeable symptoms; may include swelling of hands or face, weight gain | Severe headaches, changes in vision, light sensitivity, fatigue, nausea/vomiting, infrequent urination, abdominal and back pain |
| Organ Involvement | Indicates potential kidney involvement | Significantly affects kidneys and liver; may cause fluid in the lungs, decreased platelet count |
| Risk to mother and baby | Requires monitoring to prevent progression | Immediate medical attention is required due to high risk |
| Treatment | Regular monitoring; may include medication to manage blood pressure | Hospitalization, medication for blood pressure and preventing seizures, potential early delivery |
What are the symptoms and signs of preeclampsia during pregnancy?
Preeclampsia during pregnancy manifests in varying degrees of severity, and understanding its symptoms is crucial for timely diagnosis and treatment.
The symptoms can be categorized into those associated with mild and severe preeclampsia, which is elaborated below.
Symptoms of mild preeclampsia
Mild preeclampsia may not present noticeable symptoms, making regular prenatal check-ups essential.
Dr. Christina Buchanan, an obstetrician with Providence St. Jude Medical Center, explains on verywellfamily.com.
“The first sign of preeclampsia may be elevated blood pressure at the doctor’s office along with protein in the urine.”
She further added that:
“Blood pressure greater than 140/90 and urine protein greater than or equal to 300 mg/24 hours can indicate mild preeclampsia.”
To summarize, symptoms of preeclampsia are added below.

Symptoms of severe preeclampsia
Severe preeclampsia presents more significant symptoms, yet they often become noticeable only after some organ damage has already occurred.
According to Dr. Sherry Ross from Providence Saint John’s Health Center:
“When a pregnant person’s blood pressure is greater than 160/110 and urine proteinuria measures at 3+ or higher on a urine dipstick, a diagnosis of severe preeclampsia may be made.”
Dr. Ross further noted:
“Severe preeclampsia can lead to maternal seizures, placental abruption, and fetal and maternal death, so early diagnosis and intervention are a matter of life and death.”
Despite its risky nature, a few symptoms as mentioned below, can help with early diagnosis and effective treatment.

What are the causes and risk factors of preeclampsia?
The causes and risk factors of preeclampsia are multifaceted, with several conditions and circumstances increasing the likelihood of its development during pregnancy.
Mayo Clinic has conducted a comprehensive review of the causes and risk factors. According to their findings, below are some of the factors to watch out for if you’re pregnant.
Previous preeclampsia
Women who have experienced preeclampsia in past pregnancies are at a higher risk.
Multiple gestation
Having more than one baby (such as twins or triplets) increases the risk.
Chronic high blood pressure
Women with a history of hypertension before pregnancy are more susceptible.
Diabetes
A person with pre-existing diabetes has an increased risk of preeclampsia.
Kidney disease
Pre-existing kidney disease can elevate the risk of developing preeclampsia.
Autoimmune disorders
Conditions like lupus can increase the likelihood of preeclampsia.
In-vitro fertilization
Women who conceive through IVF may have an increased risk.
One of the major risk factors is the inconsistency in national guidelines for fetal surveillance in preeclamptic pregnancies.
A 2019 study published by Prof. Rachel Fox and her group in the Journal of Clinical Medicine, in fact, highlights this disparity and demands an evidence-based approach to figure out the right ways, timing, and how often we should evaluate this disease.
Chronic hypertension, defined as blood pressure at or above 130/80 mmHg before pregnancy or before 20 weeks of gestation, is one of the strongest independent risk factors for preeclampsia. Understanding the full spectrum of hypertension classifications, thresholds, and organ damage mechanisms helps identify which patients require the closest monitoring.
Does stress cause preeclampsia?
According to current medical understanding and research, stress does not directly cause preeclampsia.
Chronic stress may elevate blood pressure during pregnancy, increasing the risk of preeclampsia, preterm birth, and low-birthweight infants.
Research on psychological stress and preeclampsia indicates that while chronic stress affects overall cardiovascular health during pregnancy, stress alone is not established as a direct cause of preeclampsia.
Preeclampsia is believed to result from a combination of genetic, nutritional, and environmental factors, with abnormal placental development playing a significant role.
Can you have preeclampsia without high blood pressure?
Preeclampsia is typically characterized by high blood pressure, but there are instances where it can occur without this classic symptom.
Some health institutions note that pregnant women, even those without a history of high blood pressure, can develop preeclampsia and may not exhibit the more obvious symptoms associated with the condition.
Early detection remains essential because the absence of high blood pressure does not rule out preeclampsia.
The 2017 case report ‘Atypical preeclampsia – Gestational proteinuria,’ in the Journal of Family Medicine and Primary Care, presents an unusual case of preeclampsia without high blood pressure, emphasizing the importance of recognizing atypical symptoms in preeclampsia management.
Atypical presentations of preeclampsia without hypertension as a presenting feature are documented, though rare.
Atypical presentations without hypertension remain relatively rare, and further research is needed to fully characterize how preeclampsia develops in their absence.
How is preeclampsia diagnosed?
Diagnosing preeclampsia involves a combination of regular health checks and specific tests.
During prenatal visits, the doctor monitors a pregnant woman’s blood pressure, with readings of 140/90 mmHg or higher after the 20th week of pregnancy, indicating a potential concern.
The diagnostic process adheres to the criteria set by the American College of Obstetricians and Gynecologists (ACOG), outlined as follows.
A multifaceted diagnostic approach ensures thorough evaluation, which is critical for the safety of both mother and baby.
Accurate blood pressure measurement technique, including correct cuff size, patient position, and timing, determines whether a reading of 140/90 mmHg is clinically confirmed or a transient artefact. The correct blood pressure measurement technique reduces misclassification risk when monitoring for preeclampsia at home.
What are the treatment methods for preeclampsia?
The treatment for preeclampsia largely depends on the stage of pregnancy and the severity of the condition. The primary objective is to manage the health of both the mother and the fetus while mitigating risks.
According to The Eunice Kennedy Shriver National Institute of Child Health and Human Development (NIHCHD), if the pregnancy has reached 37 weeks or more, the healthcare provider typically delivers the baby to address preeclampsia and prevent additional issues.
Pregnancies under 37 weeks may allow for delayed delivery to support fetal maturation, depending on the severity of the condition.
The guidelines set by NIHCHD and various other health institutions like the Mayo Clinic and Cleveland Clinic recommend the following treatment protocol.
What are the best medications for preeclampsia?
The primary focus of medications used to treat preeclampsia is symptom management, particularly addressing high blood pressure and preventing complications.
In emergency situations involving preeclampsia, commonly employed medications include intravenous (IV) hydralazine, labetalol, and oral nifedipine.
All three medications reduce elevated blood pressure rapidly and are administered in a hospital setting under close supervision.
An article in the journal Drugs, authored by Catherine M. Brown and Vesna D. Garovic, highlights the major medications used in women diagnosed with preeclampsia.
Brown and Garovic recommend methyldopa and labetalol as first-line options for controlling high blood pressure in preeclampsia.
Methyldopa has a long history of use due to its safety profile during pregnancy, while labetalol is favored for its ability to manage blood pressure effectively without significantly impacting the fetal heart rate.
Certain medications are contraindicated in preeclampsia management.
Specifically, beta-blockers and angiotensin-converting enzyme (ACE) inhibitors are generally avoided due to their potential adverse effects on the developing fetus.
Labetalol, methyldopa, and extended-release nifedipine are the antihypertensive medications with the strongest safety evidence in pregnancy. A broader review of blood pressure medications, including their mechanisms, dosing, and contraindications, provides context for the pharmacological choices made in preeclampsia management.
Is there a cure for preeclampsia?
Currently, there is no definitive cure for preeclampsia, and the most effective treatment often involves delivering the baby, which can resolve the condition.
The decision to deliver depends on gestational age and the severity of the condition.
According to the practice bulletin titled “Gestational Hypertension and Preeclampsia” by the ACOG, managing the condition is considered best practice.
When it’s too early for safe delivery, the focus shifts to prolonging the pregnancy as long as it’s safe for both the mother and the baby.
Management includes close monitoring, antihypertensive medication, and hospitalization when clinically indicated.
Further research is needed to elucidate the root cause of this disease and gain a better understanding of the underlying causes of preeclampsia.
What are the most common complications of preeclampsia?
Preeclampsia can lead to several complications, some of which are life-threatening.
Sustained hypertension damages blood vessels, organs, and placental function, producing the complications described below.
Ian Wilkinson, a clinical pharmacologist and professor of therapeutics at Cambridge University, highlights the gravity of these complications in The Guardian.
“The two major complications in preeclampsia are stroke and prolonged fitting,” he explains.
He added:
“In preeclampsia, elevated blood pressure and leaky capillaries can cause a bleed in the brain, leading to a stroke. Additionally, inflammation in the brain can trigger seizures (fitting).”
Wilkinson notes that complications often become fatal when symptoms like severe headaches are not recognized as signs of emergency or when monitoring is not as thorough as required.
The most common complications of preeclampsia are listed below.
Stroke
Due to high blood pressure and leaky capillaries leading to bleeding in the brain.
Seizures (eclampsia)
Caused by inflammation in the brain.
HELLP syndrome
An advanced stage of preeclampsia impacting both the liver and blood.
Organ damage
Particularly to the kidneys, liver, and brain, due to elevated blood pressure.
Fetal complications
Including growth restriction, premature birth, and low birth weight.
Placental abruption
When the placenta separates from the uterus prematurely, resulting in bleeding.
Cardiovascular issues
Preeclampsia increases the risk of future heart disease.
How does preeclampsia affect the mother?
Preeclampsia significantly affects maternal health. According to a report published in BMC Pregnancy and Childbirth, it is a leading cause of maternal deaths worldwide, with higher mortality rates in pregnancies complicated by preeclampsia compared to non-preeclamptic ones.
The condition has a multifactorial origin, influenced by factors such as maternal age, pre-existing medical conditions like chronic hypertension and diabetes, obesity, and certain genetic and environmental factors.
According to NICHD, preeclampsia impacts the following aspects of maternal health.
How does preeclampsia affect the baby?
Preeclampsia can significantly impact the baby during pregnancy, leading to various complications.
According to NICHD, preeclampsia can cause problems with the placenta early in pregnancy, resulting in several effects on the fetus. The following outlines more of its impact on the baby.
The NHS emphasizes that while most cases of preeclampsia do not result in problems and often improve shortly after childbirth, there remains a possibility of severe complications.
Eclampsia, the seizure progression of preeclampsia, remains a life-threatening complication for both mother and baby, though severe cases are rare when preeclampsia is diagnosed and managed promptly.
Can you have a vaginal birth with preeclampsia?
Women with preeclampsia can indeed have a vaginal birth, although the decision between a vaginal delivery and a cesarean section depends on various factors related to the health of both the mother and the baby.
According to an American Family Physician report, about 40% of women with preeclampsia are monitored for safe vaginal delivery, while the remainder may require a cesarean section.
Clinicians base the delivery method decision on maternal condition, fetal status, and cervical readiness.
Vaginal birth remains a possibility under certain conditions, though cesarean section may be recommended when risks such as preterm birth or labor complications are present.
Particularly when the fetus has developed to 35 or 36 weeks, and the mother’s cervix is soft and prepared for delivery, natural birth can be a viable option.
In such cases, the doctor will have a detailed discussion with the pregnant woman and ensure close monitoring throughout the labor process.
Delivery planning in preeclampsia is individualized to the circumstances of each mother and baby.
Does preeclampsia go away after delivery?
Yes, the signs and symptoms of preeclampsia most often go away after delivery, typically within 6 weeks.
The NICHD emphasizes this aspect, highlighting the importance of postpartum care for women who have experienced preeclampsia.
Blood pressure associated with preeclampsia can worsen during the first few days after delivery.
Therefore, women who have had preeclampsia remain at risk for up to 6 weeks following the birth of their baby.
Postpartum preeclampsia carries a higher risk of death and requires continued monitoring and care for up to six weeks after delivery.
What is postpartum preeclampsia?
Postpartum preeclampsia is an uncommon yet severe condition marked by elevated blood pressure and excessive protein in the urine, occurring after the baby’s birth.
Unlike preeclampsia, which usually arises during pregnancy and frequently improves after childbirth, postpartum preeclampsia occurs in the period following delivery.
According to Mayo Clinic, most cases of postpartum preeclampsia develop within 48 hours of childbirth.
Late postpartum preeclampsia can occur up to six weeks or more after delivery.
The continuation or emergence of these symptoms in the postpartum period necessitates careful monitoring and prompt treatment.
Untreated postpartum preeclampsia can progress to seizures and other life-threatening complications.
The condition poses significant health risks and requires immediate medical intervention to prevent potentially life-threatening complications for the new mother.
Women and healthcare providers need to be aware of and responsive to any signs of preeclampsia that occur after delivery.
Will preeclampsia happen again in future pregnancies?
Preeclampsia can recur in future pregnancies, with recurrence risk varying widely between 13% and 65%.
According to preeclampsia.org, the recurrence risk of preeclampsia in subsequent pregnancies ranges broadly from 13% to 65%.
Recurrence risk varies by ethnicity, geographical region, and the nature of clinical interventions in the prior pregnancy.
A European Journal of Obstetrics & Gynecology and Reproductive Biology publication provides additional insights, stating that certain supplements or medications might reduce the likelihood of recurring preeclampsia.
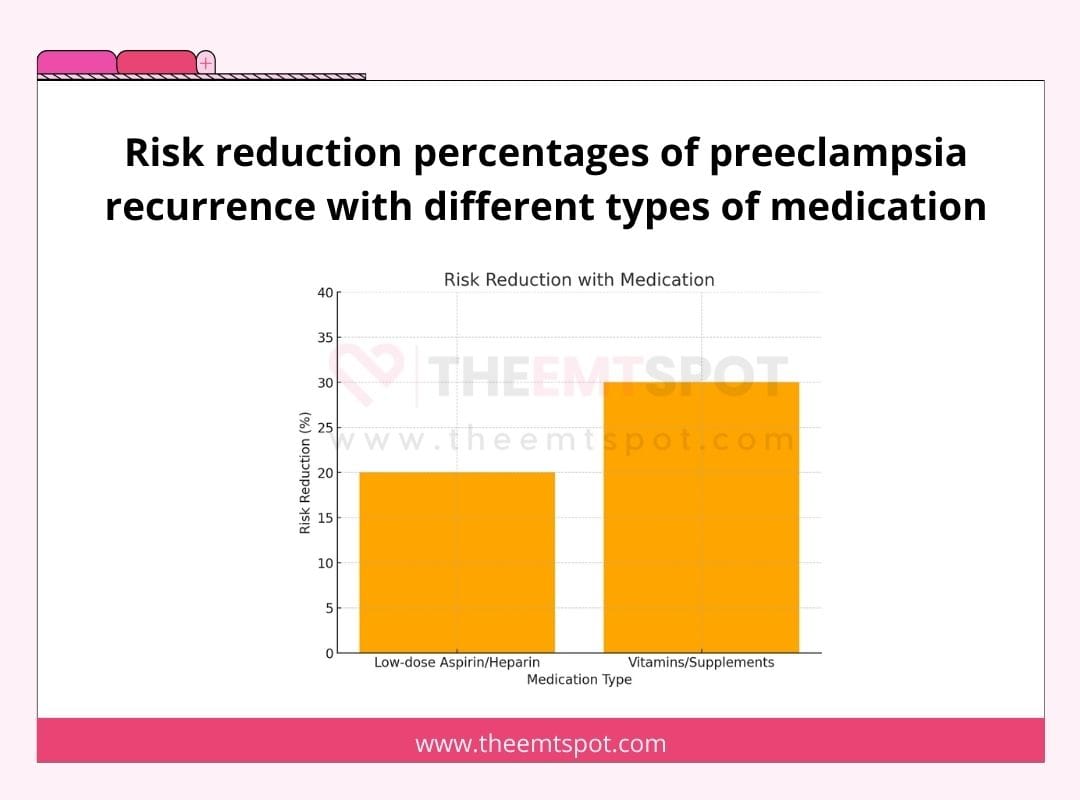
For instance, the use of low-dose aspirin or heparin has been shown to lower the risk of recurrent preeclampsia by 20% to 30%.
Vitamin D, omega-3 fatty acids, calcium, and folic acid supplementation may decrease the risk of recurrence.
Magnesium supplementation has been found to reduce the risk of pregnancy-induced hypertension in some cases.
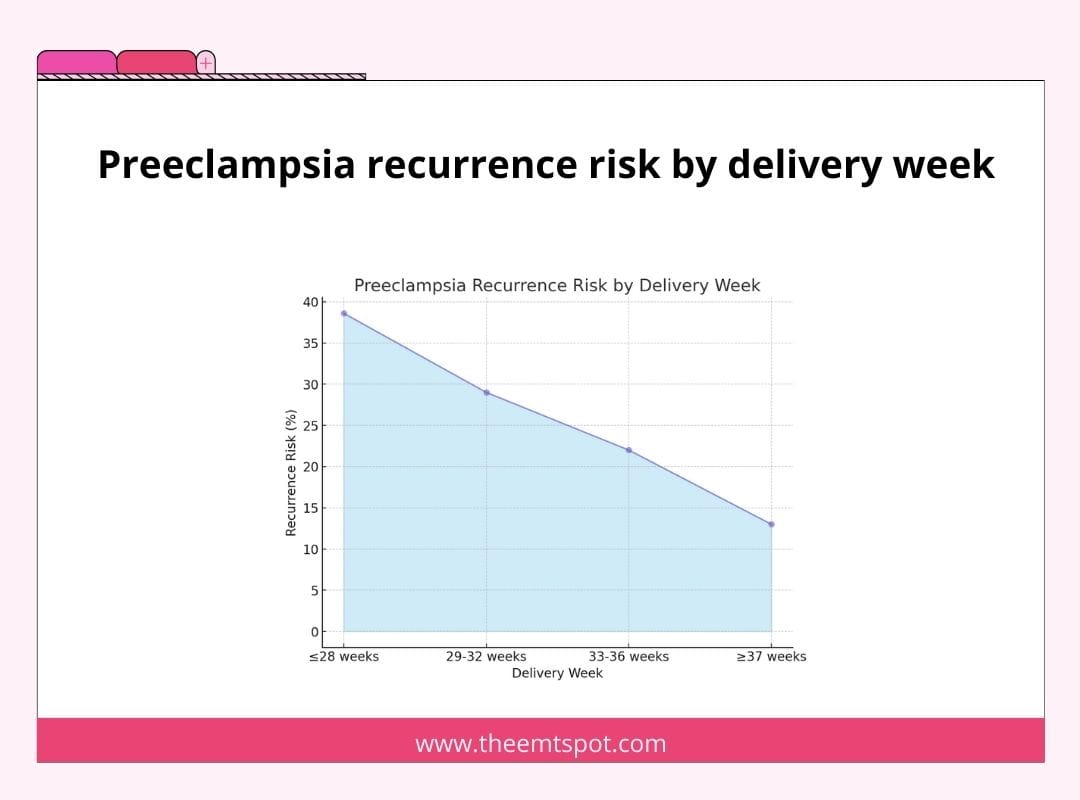
The timing of the first delivery influences recurrence risk.
Recurrence risk is highest at 38.6% when the first delivery occurred at or before 28 weeks of gestation.
Recurrence risk decreases with later delivery: 29% for deliveries at 29–32 weeks, 22% for 33–36 weeks, and 13% for deliveries at 37 weeks or later.
The earlier preeclampsia occurs in a previous pregnancy, the greater the risk in subsequent pregnancies.
How to prevent preeclampsia during pregnancy?
Preventing preeclampsia during pregnancy involves adopting a range of health strategies, according to current clinical evidence.
Key among these is dietary management, particularly for women on low-calcium diets.
High-dose calcium supplementation has been identified as potentially beneficial in reducing the risk of preeclampsia.
Shireen Meher, a consultant in maternal-fetal medicine at Birmingham Women’s and Children’s NHS Foundation Trust, UK, highlights a review of clinical trials that demonstrated a reduction in preeclampsia risk by about 36% with high-dose mineral supplementation.
Meher notes the need for caution, stating:
“The quality of this data was considered relatively low because of significant variations in the underlying risk of preeclampsia in the women who participated in the trials, meaning that more evidence is needed.”
Meher explains the rationale behind this approach:
“It’s thought that low calcium might raise blood pressure by triggering the release of hormones like the parathyroid hormone and renin. Giving calcium supplements might reduce this hormone release and prevent blood vessel constricting, leading to hypertension.”
In addition to dietary adjustments, regular prenatal care is crucial for early detection and management of signs of preeclampsia.
Adopting a healthy lifestyle, including regular exercise, healthy weight maintenance, and avoiding tobacco and excessive alcohol, contributes to preeclampsia prevention.
Monitoring blood pressure regularly can aid in the early detection and management of hypertension, a key factor in preeclampsia.
Sodium reduction, increased potassium intake, aerobic exercise, and weight management each produce clinically measurable reductions in systolic blood pressure. The evidence-based interventions covered in the how to lower blood pressure section are directly applicable to women in the elevated or stage 1 range who are trying to reduce their preeclampsia risk before or during pregnancy.
Does aspirin really help to prevent preeclampsia?
Yes, aspirin does help in preventing preeclampsia. This is supported by both the U.S. Preventive Services Task Force (USPSTF) and the American College of Obstetricians and Gynecologists (ACOG), who recommend daily low-dose aspirin (81 mg) for women at high risk of developing preeclampsia.
Starting from the 12th week of pregnancy, there is a modest decrease in the likelihood of preeclampsia observed in high-risk women without causing adverse outcomes for the fetus, increasing maternal bleeding, or leading to placental issues.
Low-dose aspirin offers the greatest benefit for women with a prior history of preeclampsia, particularly those who delivered preterm.
As explained below, aspirin is most suitable for specific groups of pregnant women.
Aspirin should be administered between the 12th and 28th weeks of gestation, preferably before 16 weeks, and continued daily until delivery.
The review by USPSTF found no significant difference in bleeding problems, such as maternal hemorrhage, fetal brain bleeding, or early separation of the placenta from the uterine wall, between the aspirin and placebo groups.
Low-dose aspirin use during pregnancy does not increase the risk of serious bleeding complications, including maternal hemorrhage or placental abruption.
Beyond aspirin, calcium, vitamin D, and omega-3 supplementation have been studied as adjunctive prevention strategies in high-risk pregnancies. A full evidence review of blood pressure supplements covers the clinical data on each compound, including dosing and populations most likely to benefit.
Why is it important to monitor blood pressure when you have preeclampsia?
Monitoring blood pressure is crucial when you have preeclampsia because it helps effectively manage and control the condition.
A 2023 study published in BMC Pregnancy and Childbirth by Atluri et al. reported that home-based monitoring improves patient outcomes and reduces risks for both the mother and the baby.
Regular monitoring allows for the early detection of any significant changes in blood pressure, which is vital for preventing severe complications associated with preeclampsia, such as stroke, organ damage, and eclampsia (seizures).
High blood pressure is a key indicator of the severity and progression of preeclampsia, and keeping it in check is essential for the health and safety of both the mother and the baby.
Women with preeclampsia can use home blood pressure monitors to track readings between prenatal visits.
A systolic reading of 140 mmHg or higher on a home monitor warrants immediate contact with a healthcare provider, as it crosses the threshold defined by ACOG for severe-range preeclampsia. The blood pressure chart shows where any reading falls relative to normal, elevated, and hypertensive ranges during pregnancy.
Home monitors allow regular blood pressure checks without requiring frequent clinical visits.
Choosing a clinically validated upper-arm monitor and following measurement instructions carefully is essential for accurate readings.
To maintain consistency, blood pressure should be recorded simultaneously each day, preferably in a seated position.
Recorded readings should be shared with the healthcare provider at each prenatal visit to guide the preeclampsia management plan.
Home monitoring supplements regular prenatal care rather than replacing it, and any significant blood pressure changes should be communicated to a healthcare professional immediately.
What blood pressure monitor should pregnant women buy?
Selecting a clinically validated upper-arm blood pressure monitor is the most important step in home-based preeclampsia management.
The key to choosing the right monitor is to look for one that provides reliable readings.
When selecting the best blood pressure monitor, it’s crucial to consider several factors to ensure accurate and reliable readings, especially for specific populations such as seniors, pregnant women, or children.
Firstly, wrist and finger monitors are generally not recommended as they provide less reliable readings than upper arm monitors.
Choosing a monitor that has been clinically validated for accuracy is essential. If you’re uncertain about the validation of a monitor, consult a healthcare professional or pharmacist for guidance.
For specific populations like seniors, pregnant women, or children, ensure that the monitor is validated for these conditions, as their blood pressure monitoring needs can differ.
Lastly, the fit of the cuff is critical for accurate measurement. Measure the perimeter of your biceps and select a monitor with a cuff size that matches your measurement.
A properly fitting cuff is key to obtaining accurate readings and is a vital consideration in choosing the best blood pressure monitor.
More in this topic